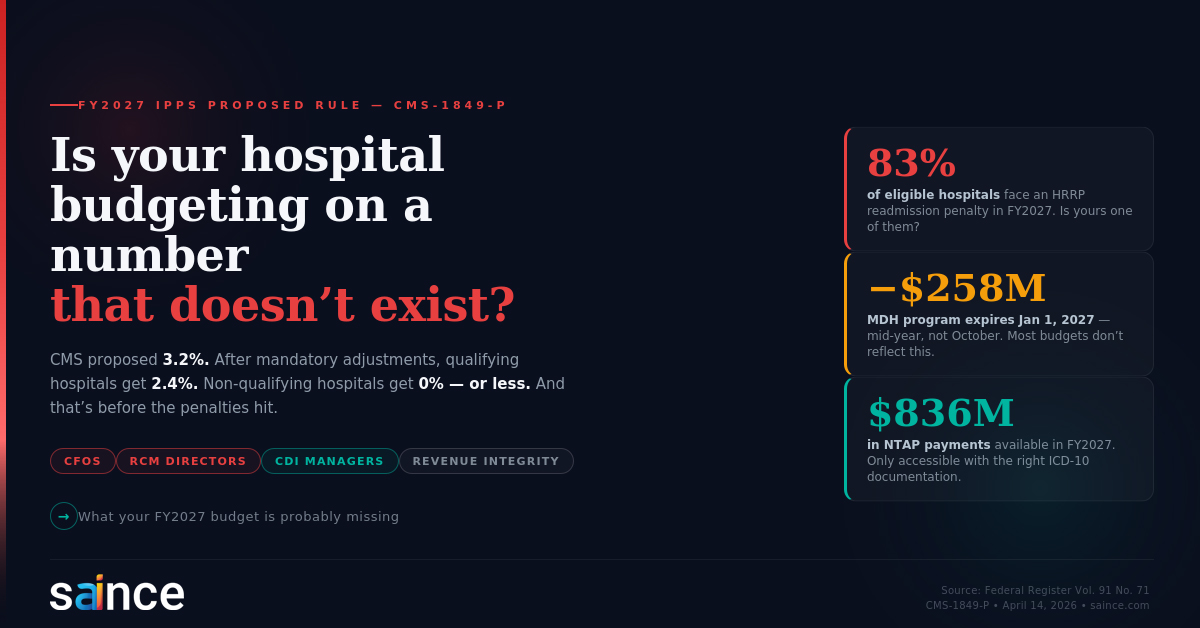
Is your hospital budgeting on a number that doesn't exist?
The FY2027 IPPS Proposed Rule: What the Payment Numbers Don't Tell You — and Why CDI Has Never Mattered More
On April 14, 2026, CMS published the FY2027 Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital Prospective Payment System (LTCH PPS) Proposed Rule in the Federal Register (Vol. 91, No. 71, CMS-1849-P). At 576 pages, this is one of the most consequential annual rulemakings in healthcare finance — and like every year, the headline number risks obscuring what hospitals will actually experience.
Here is what CDI Managers, RCM Directors, and hospital finance leadership need to understand before October 1, 2026.
The Payment Rate: One Number, Four Different Realities
CMS is proposing a market basket rate-of-increase of 3.2 percent for FY 2027, based on IGI's fourth quarter 2025 forecast of the 2023-based IPPS market basket. Before that number generates any budget optimism, it needs to be reduced by the 0.8 percentage point productivity adjustment mandated under the Affordable Care Act.
That leaves a 2.4 percent net applicable percentage increase — but only for hospitals that meet both conditions: submitting quality data under Section 1886(b)(3)(B)(viii) of the Act, and demonstrating meaningful use of certified EHR technology under Section 1886(b)(3)(B)(ix).
Hospitals that do not meet both conditions face materially different outcomes, as set out directly in the proposed rule:
- Hospital that submits quality data but is not a meaningful EHR user: 0.0% net update
- Hospital that does not submit quality data but is a meaningful EHR user: 1.6% net update
- Hospital that submits neither: −0.8% net update
This is not a footnote. It is the operative payment reality for a significant number of hospitals. CMS's own impact analysis estimates the aggregate effect of all proposed changes would increase payments to acute care hospitals by approximately $1.9 billion in FY 2027 — but that aggregate masks wide variation by hospital type, geography, and program participation.
For RCM Managers building FY2027 revenue projections: the applicable rate for your hospital depends entirely on your quality reporting and EHR attestation status. Model accordingly.
The Programs That Move Money: What's Actually Changing
Hospital Readmissions Reduction Program (HRRP)
CMS is proposing to add a new measure to the HRRP: the Hospital 30-Day, All-Cause, Risk-Standardized Readmission Rate Following Sepsis Hospitalization. This measure would have an early look beginning with the FY 2028 program year, with full use beginning in the FY 2029 program year.
The HRRP's existing financial reach is significant. The proposed rule's impact analysis shows that for FY 2027, 2,358 out of 2,832 eligible hospitals — more than 83 percent — are projected to receive a readmission penalty. The average penalty as a share of payments across all hospitals is estimated at 0.48 percent. For the hospitals penalized most heavily (those with Medicare utilization between 50 and 65 percent), the average change in payments is projected at −6.8 percent, and for those with utilization above 65 percent, −7.8 percent.
For CDI and quality leaders: sepsis documentation is now a readmission risk variable. The specificity of the sepsis diagnosis, the documentation of the clinical course, and the accuracy of discharge disposition coding all feed directly into whether a readmission is attributed to your hospital under this measure. CDI programs that have not yet built a sepsis documentation workflow should treat this proposal as the starting gun.
Hospital Value-Based Purchasing (VBP) Program
The proposed rule includes no net financial impact to the VBP program for the FY 2027 payment year — the program is budget neutral by statute. However, CMS is proposing to modify five condition-specific and procedure-specific mortality measures beginning with the FY 2032 program year, including:
- Hospital 30-Day, All-Cause, Risk-Standardized Mortality Rate Following Acute Myocardial Infarction (AMI)
- Hospital 30-Day, All-Cause, Risk-Standardized Mortality Rate Following Heart Failure
- Hospital 30-Day, All-Cause, Risk-Standardized Mortality Rate Following Pneumonia
- Hospital 30-Day, All-Cause, Risk-Standardized Mortality Rate Following COPD
- Hospital 30-Day, All-Cause, Risk-Standardized Mortality Rate Following CABG Surgery
Additionally, CMS is proposing to modify three claims-based complication measures beginning with the FY 2028 payment determination: Excess Days in Acute Care after Hospitalization for AMI, for Heart Failure, and for Pneumonia.
These are not distant concerns. The FY 2028 measures use performance data from periods that begin well before October 2026. Documentation of AMI, heart failure, pneumonia, and COPD encounters today — the specificity of the principal diagnosis, the capture of relevant complications and comorbidities, the clinical accuracy of the discharge summary — determines where your hospital lands on these measures in the coming payment years.
Hospital-Acquired Condition (HAC) Reduction Program
CMS is proposing to adopt five modified risk-standardized mortality measures into the HAC Reduction Program beginning with the FY 2028 payment determination, replacing three current measures. Also proposed: removal of three eCQMs beginning with the FY 2030 payment determination — the Venous Thromboembolism Prophylaxis (VTE-1), the Intensive Care Unit VTE Prophylaxis (VTE-2), and the Discharged on Antithrombotic Therapy (STK-02) measures.
Hospital Inpatient Quality Reporting (IQR) Program
Three new quality measures are proposed for the IQR:
- Excess Days in Acute Care After Hospitalization for Diabetes — beginning with the FY 2029 payment determination
- Advance Care Planning eCQM — beginning with the FY 2030 payment determination
- Hospital Harm–Postoperative Venous Thromboembolism eCQM — beginning with the FY 2030 payment determination
The Advance Care Planning eCQM, in particular, represents a documentation domain that many CDI programs have not yet operationalized. Advance care planning conversations are clinical interactions that must be documented in the medical record with specificity — who participated, when, what was discussed — to qualify as a reportable measure. This is a CDI function, even if it has not traditionally been framed that way.
The MDH Expiration: A $258 Million Hit to Rural Hospitals
One of the most immediately impactful provisions in this proposed rule affects a specific and financially vulnerable hospital category. The Medicare-Dependent Small Rural Hospital (MDH) program is set to expire for discharges occurring on or after January 1, 2027, under current law.
Under the MDH program, qualifying hospitals received the higher of the IPPS Federal rate or a hospital-specific rate. Beginning January 1, 2027, absent a change in law, these hospitals will be paid entirely at the standard IPPS Federal rate.
CMS estimates that the expiration of temporary changes to the low-volume hospital payment policy — which is related but distinct — would decrease aggregate low-volume hospital payments by approximately $258 million in FY 2027, affecting approximately 589 providers that are expected to no longer qualify under the post-expiration criteria.
For hospitals in this category, revenue cycle leadership needs to model this change immediately. The MDH differential has been a meaningful component of net revenue for qualifying hospitals, and the loss of it beginning in January — not October — creates a mid-year budget exposure that requires proactive planning.
MS-DRG Recalibration and Budget Neutrality
The proposed rule includes annual MS-DRG reclassification and recalibration for FY 2027, consistent with CMS's ongoing methodology. The proposed MS-DRG Reclassification and Recalibration Budget Neutrality Factor is 0.998687 — slightly less than 1.0, meaning the recalibration itself has a small aggregate negative effect on standardized amounts, offset by the budget neutrality requirement under statute.
For CDI programs, the practical significance of annual MS-DRG recalibration is this: the relative weight of any given DRG — which directly determines payment — changes every year. A diagnosis your team has been reliably capturing at a certain weight may carry a different weight in FY 2027. CDI programs that do not systematically review annual weight changes against their most frequently coded diagnoses are operating with a lag that costs real revenue.
New Technology Add-On Payments: $836 Million in FY 2027
CMS is proposing to continue New Technology Add-On Payment (NTAP) status for 41 technologies in FY 2027, with an aggregate estimated total impact of approximately $836 million. Technologies range from CAR T-cell therapies to cardiac monitoring devices to novel antimicrobials.
For CDI programs at hospitals using any of these technologies, the NTAP linkage is direct: the add-on payment is only triggered when the appropriate ICD-10-PCS procedure code — or in some cases, the ICD-10-CM diagnosis code — is present on the claim. Documentation must be specific enough to support the code. Vague or non-specific operative or procedure notes do not get the payment. This is precisely where concurrent CDI review adds financial value that is entirely separate from DRG optimization.
The TEAM Model and CJR-X: New Mandatory Episodes Beginning October 1, 2027
CMS is proposing to test and expand two episode-based payment models with direct implications for hospital documentation and care coordination:
TEAM (Transforming Episode Accountability Model): A mandatory 5-year model that would begin October 1, 2027 for acute care hospitals in mandatory CBSAs. TEAM holds hospitals financially accountable for the cost and quality of care across episodes beginning with one of five surgical procedures: coronary artery bypass graft, lower extremity joint replacement, major bowel procedure, surgical hip/femur fracture treatment, and spinal fusion. The episode extends 90 days post-discharge.
CJR-X (Comprehensive Care for Joint Replacement Expanded): CMS is proposing to expand the CJR model nationally, beginning October 1, 2027, covering lower extremity joint replacement episodes across both inpatient and outpatient settings.
For CDI and RCM leaders at hospitals in mandatory TEAM markets, this is not a FY2027 issue — it is a FY2027 preparation issue. Risk stratification in episode-based models depends entirely on how accurately a patient's clinical complexity is documented and coded at the index admission. Comorbidity capture, principal diagnosis accuracy, and procedure specificity all influence the benchmark against which your hospital's episode performance will be measured. Incomplete documentation at the index admission means your risk-adjusted target price will be set too low — and your hospital will bear the financial consequence of that inaccuracy across the entire 90-day episode.
Wage Index: Transition and Discontinuation of the Low Wage Index Policy
The proposed rule continues the FY 2027 wage index update using wage data from cost reporting periods beginning in FY 2023, with the proposed 2022 Occupational Mix Survey adjustment applied. CMS is also proposing a transition policy for the discontinuation of the low wage index hospital policy — a policy that had provided wage index increases to hospitals in areas with below-average wage indexes.
Hospitals in affected wage index areas need to model the impact of this transition on their labor-related payment components. The wage index directly affects the labor-related share of the standardized amount (proposed at 66.0 percent for FY 2027 for hospitals with wage indexes above 1.0, and 62 percent for those at or below 1.0), which means wage index changes translate dollar-for-dollar into changes in operating payments.
What This Means for CDI Programs: Five Priorities Before October 1
The FY2027 IPPS Proposed Rule, read in full, points to five clear operational priorities for CDI programs between now and the October 1 effective date:
1. Audit your quality data submission status and EHR attestation. The difference between a 2.4% update and a 0.0% or negative update is not a clinical issue — it is an administrative and compliance issue. Confirm your hospital's status for both requirements and escalate any risk immediately.
2. Build a sepsis documentation workflow now. The proposed addition of the Sepsis Readmission measure to the HRRP means that sepsis documentation quality will carry readmission risk weighting beginning in the FY 2028 program year. Concurrent CDI review of sepsis encounters — ensuring that the clinical criteria for sepsis are documented, the source of infection is specified, and the clinical response is captured — needs to begin now, not when the measure is finalized.
3. Review your FY 2027 MS-DRG weight changes against your top diagnoses. Every year, MS-DRG weights shift. Every year, some hospitals discover post-implementation that their most frequently coded diagnoses have changed weight. Schedule a systematic pre-implementation review before October 1.
4. Map your NTAP-eligible technologies to your CDI query and coding workflows. For each of the 41 proposed NTAP technologies used at your hospital, confirm that your CDI and coding processes reliably capture the required codes. The $836 million aggregate NTAP pool is only accessible to hospitals whose documentation supports the required specificity.
5. Prepare for TEAM if you are in a mandatory CBSA. Begin now with comorbidity capture audits for CABG, joint replacement, bowel resection, hip/femur fracture, and spinal fusion cases. Your risk-adjusted target prices under TEAM will be set based on how accurately these patients' complexity is documented at the index admission.
What This Means for RCM Managers and Directors
Model net revenue at your actual applicable percentage increase, not the headline market basket figure. The 3.2% market basket is reduced to 2.4% for qualifying hospitals — and potentially to 0.0% or below for those with quality reporting or EHR attestation gaps.
Account for MDH expiration in January if applicable. The MDH payment differential ends January 1, 2027, not October 1. Budget models that treat FY2027 as a uniform full-year rate will be wrong.
Quantify your HRRP penalty exposure. With 83 percent of eligible hospitals projected to receive a readmission penalty averaging 0.48 percent of payments, HRRP is a material revenue risk for most hospitals. CDI investment that reduces preventable readmission attribution is a net revenue strategy, not just a quality initiative.
Factor in low-volume hospital payment policy changes. If your hospital has been receiving the low-volume hospital payment adjustment, confirm whether you qualify under the post-January 2027 criteria — which revert to the original statutory methodology from the FY 2005-2010 period.
The Bottom Line
The FY2027 IPPS Proposed Rule will be finalized in August 2026 and takes effect October 1 — with some provisions, including the MDH expiration, taking effect January 1, 2027. The preparation window is open now.
The organizations that will navigate this rule successfully are those that read past the headline number and address the specific operational levers the rule actually contains: quality program reporting compliance, documentation-driven sepsis readmission risk, NTAP code capture, MS-DRG weight changes, and — for hospitals in mandatory markets — the episode-based accountability that begins with TEAM in FY2028.
Clinical documentation is the foundation of every one of these levers. It determines your applicable payment rate category, your readmission measure performance, your quality measure reporting results, your NTAP eligibility, and your risk-adjusted episode benchmarks. In the FY2027 environment, CDI is not a billing function. It is the clinical data infrastructure that determines whether your hospital captures the revenue it earns and avoids the penalties it can prevent.
Saince provides AI-powered CDI software designed to help hospitals achieve documentation accuracy at scale — from concurrent CDI and physician query management to MS-DRG impact analysis and quality measure documentation workflows. To learn how Saince can help your team prepare for FY2027, contact us at sales@saince.com.
Source: Federal Register, Vol. 91, No. 71, April 14, 2026. Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals (IPPS) and the Long-Term Care Hospital Prospective Payment System and Policy Changes and Fiscal Year (FY) 2027 Rates; Requirements for Quality Programs; and Other Policy Changes. CMS-1849-P.